
Flexor Tenosynovitis
- Cosimo Laterza

- Sep 23, 2019
- 2 min read
Updated: Sep 24, 2019
Flexor Tenosynovitis, an infection of the synovial sheath that surrounds the flexor tendons, is an ORTHOPAEDIC EMERGENCY!!!!
Learn all about Flexor Tenosynovitis to adequately diagnose and treat this threatening disease.
Epidemiology and Risk Factors
Flexor Tenosynovitis has an incidence of up to 9.5% of all hand infections.
Leading risk factors include diabetes, IV drug use and immunocompromised patients.
Anatomy
The flexor tendons are enclosed in three types of sheaths as seen in the photo below.
The sheaths are all connected to the deep spaces of the hand and can lead to further systemic infection, which is why this condition is considered an orthopaedic emergency.
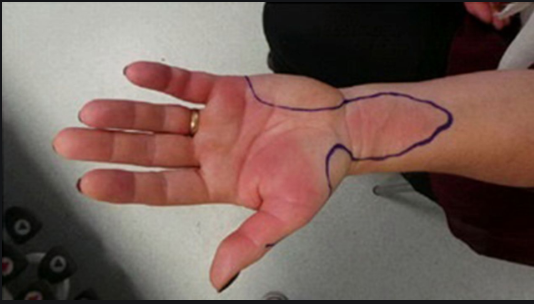
It is important to note that one important complications is the horseshoe abscess (photo below). This occurs because of the spread of infection from the ulnar flexor tendon sheath to the radial flexor tendon sheath due to their close proximity to each other.

Pathophysiology
Flexor Tenosynovitis often occurs due to a penetrating trauma to the tendon sheath.
Mechanism can also occur from direct spread from other sources of infection including a felon, septic joint or deep space infection.
Most common organism is Staph Aureus, with less common being MRSA (IV drug abusers) , common skin flora, Eikenella (human bites) and Pastuerlla multocida (animal bites).
Symptoms
See below an amazing picture describing Kanavel Signs, a great physical exam tool to diagnose this condition.
According to a HAND: Sage Journal article from 2017 these signs ranged from 91.4% to 97.1% in sensitivity while specificity ranged from 51.3% to 69.2% .

Work Up
CBC to check WBC.
ESR to check inflammatory status.
Ultrasound for the ability to look at a fluid collection between tendon and bone.
Xray to rule out any underlying osteomyelitis.
Video Time!!! Check out a portion of this awesome video from our friends at Massachusetts General Hospital! Watch from 2:21-4:09 where the video reveals the technique and signs to look for on ultrasound.
Management
Flexor Tenosynovitis is an emergency and it should be treated as such.
These patients will require emergent hand surgery consult in the ED with immediate IV antibiotic therapy that normally includes Vancomycin with Unasyn or Zosyn or cefoxitin.
Patients will be admitted and sent to the operating room for an incision and drainage with washout followed by culture-specific IV antibiotics.
Video Time!!! See this amazing video by Dr. Marshall Murdoch. This will demonstrate the correct washout technique which entails performing two small incisions, one placed distally at the A5 pulley and one placed proximally at the A1 pulley. Water is then flushed through the area using an angio-catheter.
Review Time!
Check out this quick #EMin5 video by Dr. Anna Pickens below that provides a great overview of the topic.
References
“Pyogenic Flexor Tenosynovitis.” Orthobullets, www.orthobullets.com/hand/6105/pyogenic-flexor-tenosynovitis.
“Flexor Tenosynovitis.” WikEM, www.wikem.org/wiki/Flexor_tenosynovitis.
Shah, Nikki, et al. “Acute Horseshoe Abscess of the Hand after Corticosteroid Injection to Treat Trigger Thumb.” BMJ Case Reports, BMJ Publishing Group, 29 Aug. 2018, casereports.bmj.com/content/2018/bcr-2018-225535.info.
Kennedy, Colin D, et al. “Differentiation Between Pyogenic Flexor Tenosynovitis and Other Finger Infections.” Hand (New York, N.Y.), SAGE Publications, Nov. 2017,
Peach, Mandy. “Infectious Flexor Tenosynovitis.” Department of Emergency Medicine | Saint John Regional Hospital, 11 Apr. 2019, sjrhem.ca/rcp-infectious-flexor-tenosynovitis/.www.ncbi.nlm.nih.gov/pubmed/28720000.



Comments